


Hello, Readers. Please go and read my feature in the New Westminster Times—it serves as the main article for this breaking story. Please also support Lorraine and Dave Brett’s endeavour to bring hard hitting independent local journalism back to Canada. The New Westminster Times does not received any government funds, it is an independent news outlet.
As always you can drop a tip in my By Me a Coffee Tip Jar if you found this story helpful and want more of this kind of investigative journalism.
What follows here is an article that provides supplementary information, so you can understand the real story behind the story. You will need to read both articles to really get a handle of this story.
Canadian gender clinicians downplay damage they do to the brains of children with sex hormone agonist therapy, commonly called “puberty blockers”, because the suffering of the children makes it okay for them to compromise the adolescent brain. Children requesting gender affirming care (GAC) don’t have much of a clue about anatomy and biology and hormones and reproduction. They don’t understand the gravity of GAC, they lack the developmental capacity to consent. Schools facilitate social transitioning, a medical intervention, to the extent of providing breast binders. Canadian gender clinicians treat gender confused and distressed children with a GAC approach to prevent surgeries. Children don’t have gender affirming body modification surgeries in Canada. Gender distressed female children see mastectomy and menstrual suppression as the be all end all. Skeptics and anyone who questions GAC are haters spreading disinformation and gender clinicians and gender activist NGOs must fight back.
I heard these ideas and lot more when I attended a webinar hosted by the Knowledge Mobilisation unit of Children’s Healthcare Canada (CHC) called Gender-Affirming Care for Youth: Essential Knowledge for Healthcare Providers, delivered by Vancouver-based paediatric endocrinologist, UBC faculty of medicine clinical professor, and award winning health care advocate Daniel Metzger.
You can take a look at some of the presentation slides below; note: I think I may have missed a few slides at the beginning. The public has no access to the slides, or any information about what Metzger shared in the webinar, which will only appear on the CHC member portal. Paediatric health care institutions and non profit NGOs who support them can join the CHC. The general public has no access to the member portal, despite the fact that the endeavours promoted by the Knowledge Mobilisation Unit directly impact and involve them and their children and grandchildren.
Of the 11 webinars CHC hosted last year, three focused on gender affirming care, and the association, which typically records its webinars for later viewing, recorded none of the gender webinars it hosted in 2025. Fortunately I recorded the session in its entirety for the world to hear — see the video above.
What the heck is knowledge mobilisation, reader? It sounds like an obfuscatory Woko Haram term for propaganda, doesn’t it? According to their website, “Children’s Healthcare Canada’s SPARK Knowledge Mobilization Program aims to curate and showcase knowledge, evidence (from research, practice, policy, and lived experience), and expertise to SPARK conversations, ideas, and action.”
Reader, how can the CHC spark conversations when they shut them down when their clandestine modus operandi and their censorious nature? The Metzger webinar moderator deliberately ignored the critical questions posed by audience members. Moderator’s privilege, she said as she picked the questions she would ask Metzger to answer, after he delivered his presentation.
Is Knowledge Mobilisation (KM) a progressive term for propaganda? Yes! When we take a look at the CHC website, we see that’s exactly what KM means. Propaganda describes a form of communication designed to influence public opinion through biased, skewed, and distorted information. KM becomes propaganda when it oversimplifies complex issues with the objective of influencing opinion toward a particular belief or position. That’s exactly what the CHC has done with its GAC webinar. Gender medicine activists present very ideologically skewed information as evidence for their disembodiment body modification approach to treating psychologically and emotionally distressed children and youth.
What do we know about the CHC Association? It has federal non profit status, which usually means a tax exemption.
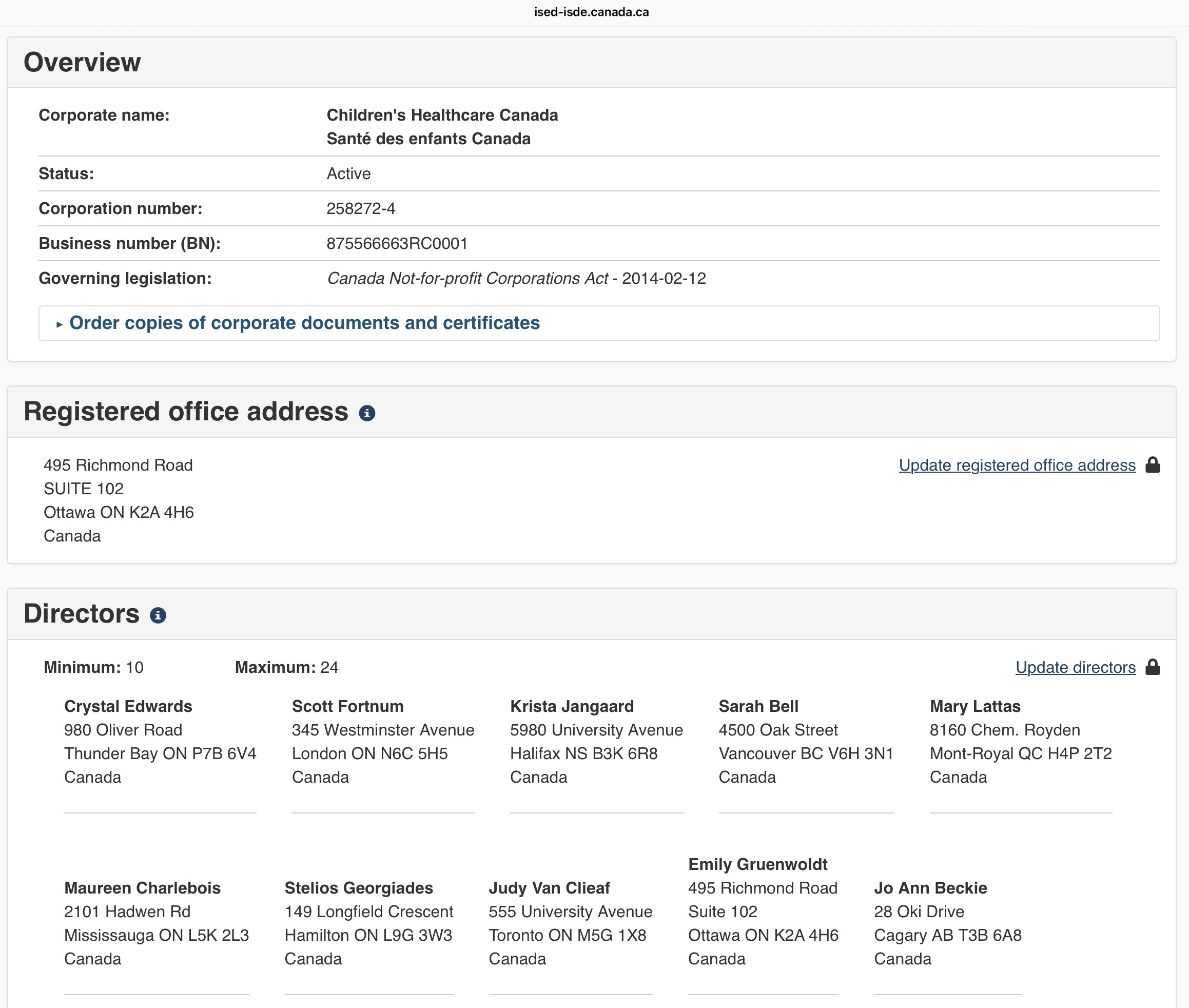
Who funds the CHC? Well, it’s unclear, because the CHC does its best to obfuscate any kind of financial accountability. CHC funding derives from a combination of philanthropic, corporate, and advocacy-driven channels. Whilst it receives no direct operational funding from the Canadian government, it actively lobbies for increased public investments in children’s healthcare. I couldn’t find any financials for the CHC, and the financial statement I could find for the CCHF didn’t reveal much. I found a list of CHC members and patrons here.
Patrons of the CHC include the Alberta Children’s Hospital Foundation, the BC Children’s Hospital Foundation, the Canada Children’s Hospital Foundation (CCHF), the CHEO Foundation, Children’s Health Foundation, The Children’s Hospital Foundation of Manitoba, the IWK Foundation, McMaster’s Children’s Hospital Foundation, Sick Kids, Stollery Children’s Hospital Foundation, Trillium Health Partners Foundation.
The CHC has a profile on the national lobbyist registry. A recent issue of the Lobby Monitor reports the CHC as the most active lobbying group on Parliament Hill during the first week of October.
In my research I did come across a list of CCHF private patrons; for fundraising, the CHC partners closely with CCHF, the largest non government funding source for child health.

In summer of 2023 I wrote about the shady way that the BC government funds the sex hormone agonist Lupron, commonly referred to as “puberty blocker,” for gender confused and distressed children and adolescents. Remember, reader, that no official clinical indication exists for Lupron to a treat paediatric gender dysphoria or discordance. It’s an off-label use.
AbbVie has no intention of applying to the FDA to expand the use of Lupron to include treatment of paediatric gender dysphoria. Health Canada has not officially supported the use of Lupron for paediatric gender affirming care. No official clinical indication exists, that’s what off-label means. If Lupron did prevent adolescent suicide don’t you think that the drug company would have gotten formal FDA approval for that as an official indication? If Lupron did relieve adolescent depression don’t you think that the drug company would have gotten formal FDA approval for that as an official indication? If Lupron did relieve adolescent self harm don’t you think that the drug company would have gotten formal FDA approval for that as an official indication? I’ll take things that will never happen, Alex. Reader, Lupron has a very controversial track record as a treatment for its clinical indications. The clinical trials supporting its FDA approval for Lupron have grave weaknesses. Google Dr. David Redwine.
In the extensive research I conducted leading up to LupronGate, I stumbled upon a website with a wealth of crucial information about Lupron, compiled by a victim of Lupron. Among the treasures I found there, I came across a damning expert report on Lupron.
“Lupron should only be limited to six injections for the initial treatment, and a retreatment should not exceed six injection. Lupron cannot be given more than twelve injections per life time.” — John Geuriguian, MD, (retired professor of pharmacology, retired Medical Officer with the US FDA), in a expert report for Karin Klein’s case against Lupron.
How many doses do Metzger and his gender medicine colleagues prescribe to gender distressed children? The story about the young Swedish female adolescent, Leo, revealed that she had received 4 years worth of Lupron doses. Now she struggles with severe bone density loss that has caused spinal fracture and vertebral malformation, she lives in extreme pain. Leo received four times the recommended lifetime dose of Lupron.
Leo was on the medication for four years and [her] bone density was never checked.
The effects were little short of catastrophic. Leo now suffers from severe osteoporosis, a weaking of bones which is normally seen in people in their 60s and 70s. It is almost irreversible. [Her] mother says that he was in pain from skeletal damage; [s]he was constantly depressed; and [s]he attempted to commit suicide several times. — Trans narrative under fire in Sweden, Michael Cook, May 7, 2022, in BioEdge
Reader, what we have here amounts to medical malpractise. I don’t think it’s hyperbolic to say that we face the biggest medical scandal in history. Which makes this webinar delivered by Metzger shocking and disturbing. Reader, many of the things Metzger said in this webinar echo what he said in the leaked WPATH transcripts, contained in Mia Hughes’ 2022 WPATH Files. Despite much evidence to the contrary that’s emerged since the WPATH Files, Metzger still insists on the reversibility of “puberty blockers.”Reader, should we ask Leo if the effects of her “puberty blocker” treatment have proved reversible?
Here’s a recent feature from Rebel News about a young women named Rose Guerin‑Test, who found herself lured into the gender body modification cult at age 13. She had a double mastectomy at 16. She’s 21 now.
Rose had insurance coverage for the double mastectomy they pressured her into at age 16, and she cannot get insurance coverage for the breast reconstruction she would like to get back what the gender cult took from her as a child. Her mother felt conflicted and thought of transitioning a mistake, the influencers on social media had more influence on Rose than her mother, and Rose made suicide threats to hasten the transition process, to get what she thought she wanted.
The two young people Rose knew who transitioned have since detransitioned. Metzger wants us to think it’s uncommon or rare to see detansitioners, and that’s misleading. Rose’s mother feels it’s professional misconduct.
Here’s the video of a recent interview with a pioneer of paediatric gender medicine Dr. Susan Bradley, conducted by Stella O’Malley and Mia Hughes.
Reader, what do you think about all this? If you want to share your thoughts and concerns, or if you have a personal experience with paediatric gender affirming care you want to share, please feel free to get in touch with me.
You can reach me at pubertyisnotadisease[at]gmail[dot]com.

