

“The Cass Review is a Pile of Garbage” — Dr Daniel Metzger
the proponents of gender affirming care continue to double down and deny the valid and reliable critical research analysis that’s emerged to challenge their claims that they’re saving kids’ lives

A considerable amount of time and care and skill goes into researching and preparing these articles that challenge gender affirming care (GAC) as a legitimate method of treatment for adolescent children experiencing distress and disembodiment related to sexual maturation. The few who do this work typically paywall their articles. I have consistently chosen not to paywall this stuff. It comes at a cost to me. I consider it a service to humanity and my country. If you appreciate this work, please consider a paid subscription or dropping a tip in the tip jar. Thank you for reading.
Parents and others with stories about their experience with paediatric GAC, and anyone with comments or concerns or criticism related to paediatric GAC they would like to share can feel free to email me at the email below.
pubertyisnotadisease@gmail.com
Nearly a month ago I attended a webinar hosted by Spark, the Knowledge Mobilisation Unit of the Children’s Healthcare Canada, and delivered by Dr. Daniel Metzger. Anticipating that CHC would choose not to record the webinar, I recorded the audio myself. I wrote lengthy pieces about what I heard Metzger say in that one hour presentation and my stories got eclipsed by the outrage over the Cowichan ruling, and also by the debate that took place between Morgane Oger and Mia Hughes, hosted by Laurier HxA, mediated by Jon Kay.
It would seem we have a cult-like response to news stories about political events and we impose a certain mutual exclusivity onto our discourse about the issues. Do algorithms drive this peculiarity? Does poor and morally bankrupt political leadership contribute to this peculiarity? Maybe it’s a popularity contest and only the cool kids get exposure, meaning a nonentity like me, who tries to stay away from the manipulation of sensationalism, can only get the leftover crumbs? I don’t know. I stubbornly continue to investigate and share what matters in this space, Adventures of Bad Hijabi, without a paywall, hoping to lead people to the reality of issues affecting them. I encourage anyone who finds this publication useful to take out paid subscriptions or drop a tip in the tip jar by clicking the tip jar button above.
Anyway, let’s get to the main point of this article, shall we?

“I don’t want to spend a lot of time on the Cass Review because it’s a pile of garbage. These are folks in the UK, for probably good reasons, because there was a bit of an upheaval in the one clinic that looked after kids, they transitioned this review, there’s so many arguments you can make against it, I think none of the authors—not all of the authors were identified but of those that were, none of them do trans care for youth, they were paediatricians but I think they were probably paediatricians who probably came with a particular mindset …” — Dr. Daniel Metzger
Here’s a clip from 2024, in which BBC Today interviewed Dr. Cass about her findings.
Video Transcript
“There has been a significant change in the population of young people over the last 10 to 15 years so about 15 years ago the service was seeing perhaps 50 predominantly birth registered Boys in childhood and over the last 10 years or so it’s switched to over 3,000 young people and it’s mainly birth registered girls presenting in early teens and as you say often with quite complex additional problems.” — Dr. Hilary Cass
“Were those additional problems addressed properly in your view?
“Well no because of the toxicity of the debate they’ve often been bypassed by local Services who’ve been really nervous about seeing them so rather than doing the things that they would do for other young people with depression or anxiety or perhaps undiagnosed autistic Spectrum Disorder they’ve tended to pass them straight on to the GIDS service and they’ve then ended up at the back of a very long waiting list because GIDS wasn’t really able to cope with the rising number and the complexity of their presentations.” — Dr. Hilary Cass
“But when you talk of the toxicity and them being passed on passed on why but for fear of being accused of being transphobic what was the reason?”
“Well we did a survey early on and I expected that clinicians would say we don’t have the time we’ve got very big backlogs but the things that they were really worried about is no guidance no evidence and no training and as well as you say worrying that if they did the usual sort of assessment that they would do for other children they would be not necessarily accused of being transphobic but not immediately affirming the young person in their gender.” — Dr. Hilary Cass
“Is there evidence that puberty blockers are safe to use?”
“No we don’t have good evidence at the moment they are absolutely safe to use for a completely different set of children which is children who go into puberty too early and they’re also used for adults with certain kinds of cancers but this is a a novel use using them to arrest puberty and we don’t know the long-term impact of that on brain development because there’s a rapid period of brain development in adolescence and we also don’t know if it changes the trajectory of somebody’s gender and psychosexual development.” — Dr. Hilary Cass
“Is it normal in medicine for something that is so unknown to be used and used so much in one area?”
“Well the team did start off by doing a clinical trial but the point at which practice diverted from the evidence was when they went on to routinely prescribing before the trial results were available and also prescribing to a wider group of young people.” — Dr. Hilary Cass
“Why do you think they did that?”
“They clearly felt that they were doing the best for this group of young people and obviously they would have seen some young people who they felt were improving but we do know once the study results were released that some young people were improving but some young people were getting worse and that’s not surprising because their broader range of problems were not being addressed it is unusual for us to give a potentially life-changing treatment to young people and not know what happens to them in adult hood and that’s been a particular problem that we haven’t had the followup into adulthood to know what the results of this are that’s the reason why I’ve said that we must improve the research base here so that means finding out what happens not just to the young people who go onto puberty blockers or on masculinizing and feminizing hormones but also those who don’t go on a hormone pathway we need to know how psychological therapies help as well.” — Dr. Hilary Cass
“You talked earlier about the initial stages of of children seeking treatment and people not wanting to GPs presumably initially not wanting to get involved and The Wider mental health staff that there are what was there also in your view and according to your report a pressure on Tavistock and on the gender identity uh clinic in particular that they were willing to accept from outside that push push them down a particular route.”
“Yes I mean I think there’ve been all sorts of pressures on everybody involved and I think people at the front line in whatever setting felt that they were of pressures on everybody involved and I think people at the front line in whatever setting felt that they were doing the right thing I mean everybody I spoke to passionately believes that they’re doing the right thing nobody’s setting out to uh to harm children um but I think one of the difficulties for the Tavistock was when there wasn’t any other Centre that that was providing the same treatments in the country you don’t have peers to to talk to and so you then um there’s less reflection perhaps.” — Dr. Hilary Cass
“I want to play you a clip if I may of a transwoman who we’ve talked to in her 20s now about the delay that she feels did her real damage when she was younger 20s let’s hear it.”
“All in all I spent four years on waiting lists to be seen by an NHS specialist it was incredibly frustrating um and the period between being told that oh we’re not going to see you before your 18th and being referred on and then me gaining uh private healthcare was an incredibly dark period in terms of my mental health it was the lowest l’ve been uh during the course of my transition because of simply me having to to wait as long as l did I went through pretty much the full course of male puberty during that time I felt incredibly uncomfortable it never felt like me I always felt wrong I didn’t feel like I could accurately be myself and that’s purely because I had to wait so long to gain any semblance of care.” — Anonymous male who identifies as the opposite sex, who wishes he would have been ‘gender affirmed’ before the effects of male puberty took effect on him
“What’s going to happen now, Dr. Cass, to the hundreds, possibly thousands, of children who are now in that position and who’ve been told certainly, on the NHS in England, there is no chance of puberty blockers and, well, nothing much happening?”
“Well first off, I’m really sorry to hear that story because it is heartbreaking and I know there are many other stories like that in the first instance NHS England has put some additional uh resource into support local services to at least be doing an initial assessment—” — Dr. Hilary Cass
“Is it enough do you think?”
“It’s not about the money, it’s about the workforce, and a huge part of this is we have got to help clinicians from all backgrounds realize that they do have the transferable skills to see these young people and I know there are massive waiting lists for mental health in general but this particular group of people has been disadvantaged compared to other similarly distressed young people.” —Dr. Hilary Cass
“The point being I suppose as well that the things that will be off offered might not include or or might be an effort to avoid the kind of things that would change a person’s body forever.”
“Yes there is going to be a small number of young people for whom a medical pathway is the right pathway and in many ways the more we can address the wider problems for some of those young people who are not going to go on a medical pathway the easier it will be for us to to ensure that those who are going to need a medical pathway get onto that specialist track sooner rather than later.”—Dr. Hilary Cass
“There are still private clinics aren’t there that are able to prescribe puberty blockers should there be everybody should be getting the same standard of care?”
“And I do have concerns about private provision which is not providing the level of assessment that I’m recommending in the NHS. I fully understand why parents have felt that going down that path is the best way to serve their children, particularly just hearing that harrowing story of a 4-year wait. We have asked NHS England to provide advice to families about what it means if they go down a private route in terms of coming back into the NHS later.”—Dr. Hilary Cass
“Has this been a medical Scandal? Is that the right way to see it?”
“I think that’s for somebody other than me to make a judgment on l’ve just been focused on the best way to move forward to get a holistic package of care for these young people to get them back into a more mainstream form of mental health and pediatric provision and to get the evidence that we need for so that they can make informed decisions in the future.”—Dr. Hilary Cass
“Dr Hillary Cass thank you very much for talking to us.”
“Thank you.” —Dr. Hilary Cass
“And um just to say the NHS have been in touch with us and said that they’re making significant progress to towards establishing that fundamentally different uh gender service for children and young people they’ve written to local NHS leaders, they say, to ask them to pause offering first appointments at adult gender clinics to young people below their 18th birthday.”
I notice a few things.
First of all, Dr. Cass seems far more serious than does Dr. Metzger about her role as a paediatric physician. She exhibited genuine concern for the paediatric patients in the GIDS which she reviewed. She also expressed empathy for the person in the clip who seemed to think receiving GAC as a young person would have relieved the suffering of that period of development and growth. When the interviewer played the clip of this trans person, it struck me that the gender affirmation movement really seeks to affirm adults who struggle with accepting their reproductive class and their body, from a primary and secondary sex characteristics perspective. The gender affirmation movement targets children and youth so fanatically because the adults driving the movement struggle with disembodiment and they believe in stopping puberty as the cure for their disembodiment and inability to accept the sexuality of their body. The gender affirmation movement lives vicariously through other people’s children.
Why would anyone think we can find remedy for adolescent disembodiment and self loathing in permanently altering and damaging the body to align with an almost certainly distorted adolescent self perception? This seems deeply misguided irresponsible. Metzger himself has said more than once1 that young people presenting for GAC don’t have the developmental capacity to provide informed consent for the medical pathway that GAC requires.
Did readers notice that Dr. Cass didn’t rule out a medical pathway of GAC for young people? Unlike many harsh critics of GAC, Cass didn’t make blanket statements that would point to a delegitimisation of gender identity, “trans kids”, or paediatric gender affirming care. One could hardly call her hateful or “transphobic,” as Dr. Metzger seemed to elude to in his presentation when he mentioned skeptics and whistleblowers. Dr. Cass seems quite reasonable, in comparison to Dr. Metzger. In fact, Dr. Cass suggests that providing alternative treatment algorithms for those children who don’t need or suit the medical pathway would make it easier for the children who do need and suit it. Surely that’s what the gender affirmation movement wants, isn’t it?
In the webinar, Metzger himself concedes that, there being no screening mechanism, there being no way to tell the “‘trans kids” from the “not trans kids”, means that some children will find themselves caught in the medical pathway when they don’t belong there. I find irresponsible Dr. Metzger’s nonchalance at sweeping all children into the GAC algorithm, because relieving some suffering makes it worth it. It seems transactional. It more resembles a cult than it resembles medical care for children. Why do gender affirmationists want to turn paediatric medicine into a tent revival scenario? Why do we have gender identity evangelicals fanatically promoting sex changes2 for children and adolescents?
Dr. Cass spoke about the overwhelming demand for GAC which the GIDS faced, she spoke about the genuine concerns of the clinic staff, who felt they lacked guidance in a very novel area3 of paediatric medicine. Dr. Cass also spoke about the medical complexities of the young people presenting at the Tavistock clinic. She mentioned the low quality of evidence for the GAC medical pathway, and emphasised the need for more rigourous research to support children and youth experiencing gender discordance. Dr. Cass also mentioned medical uncertainty regarding the cognitive and other long term effects of treating psychiatric distress in paediatric patients with GnRHa and cross hormones.
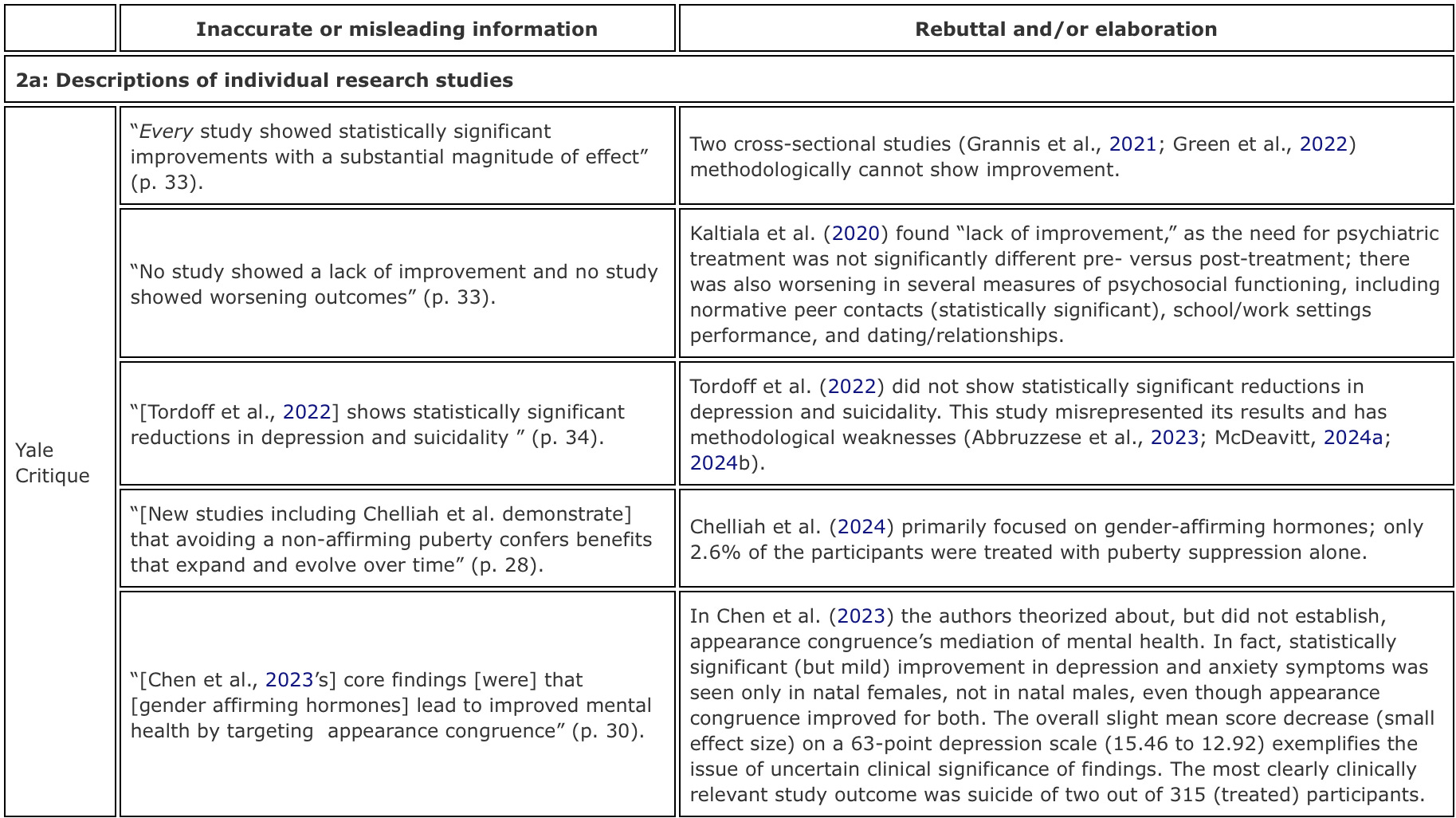
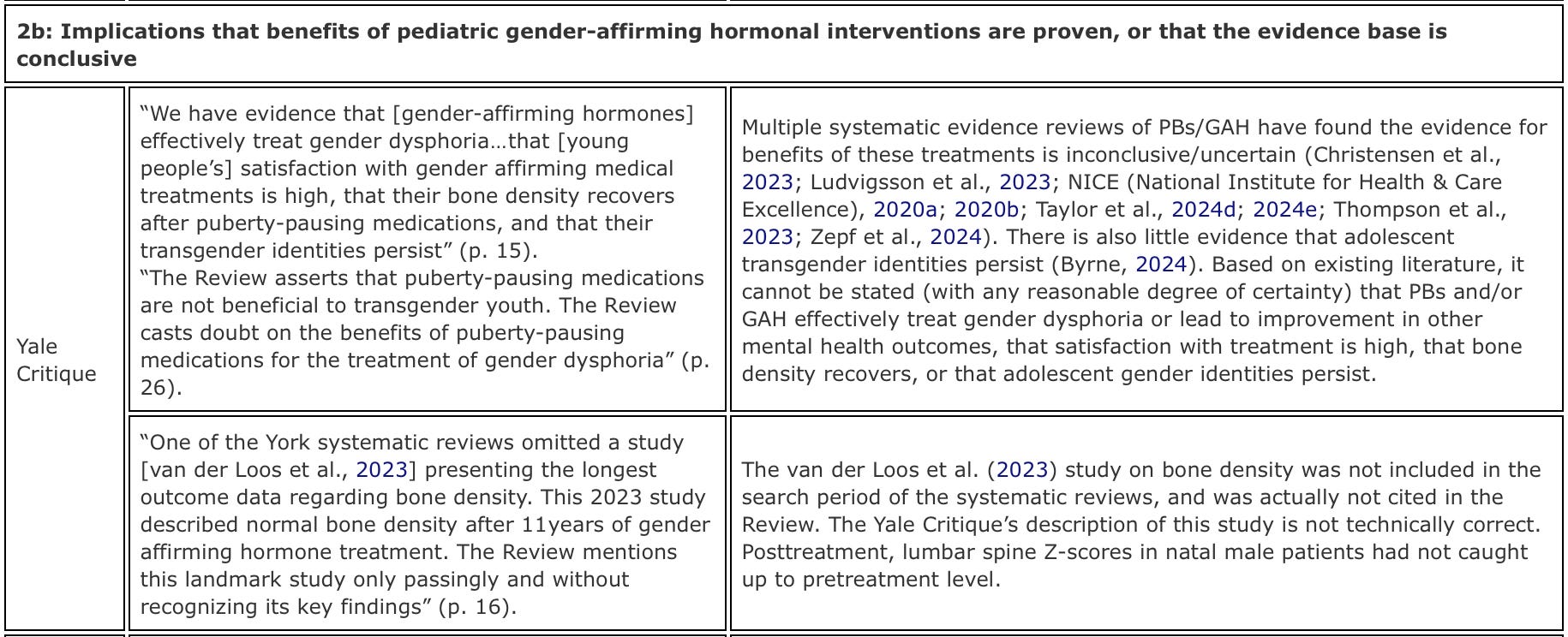
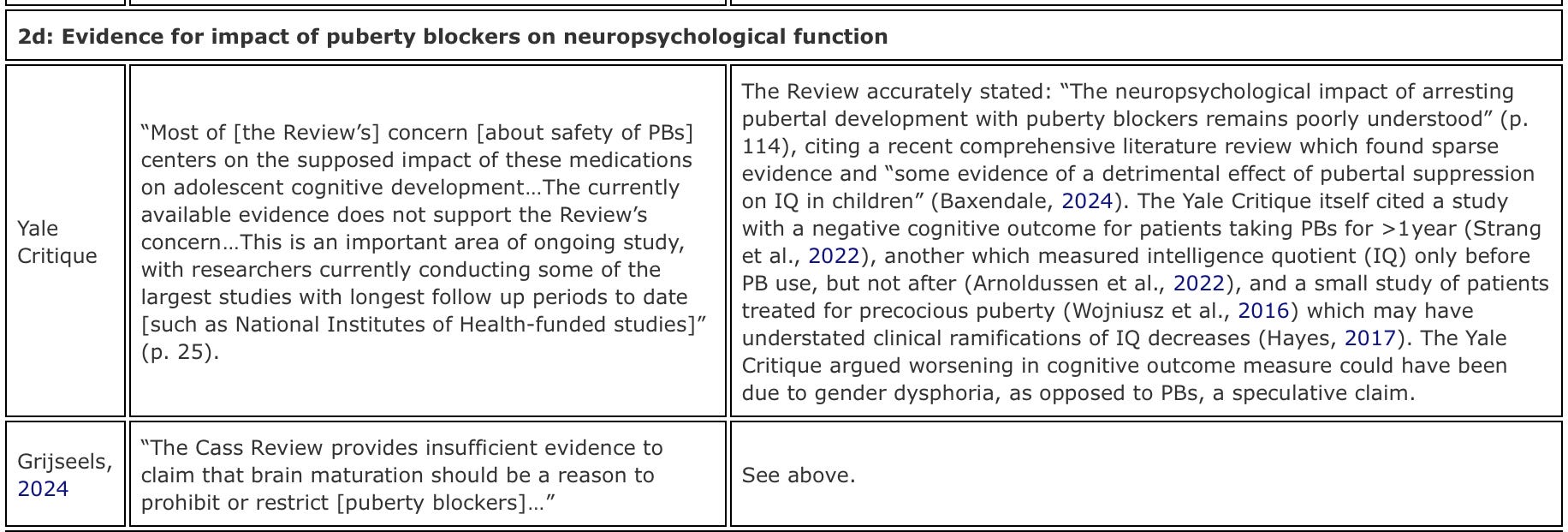
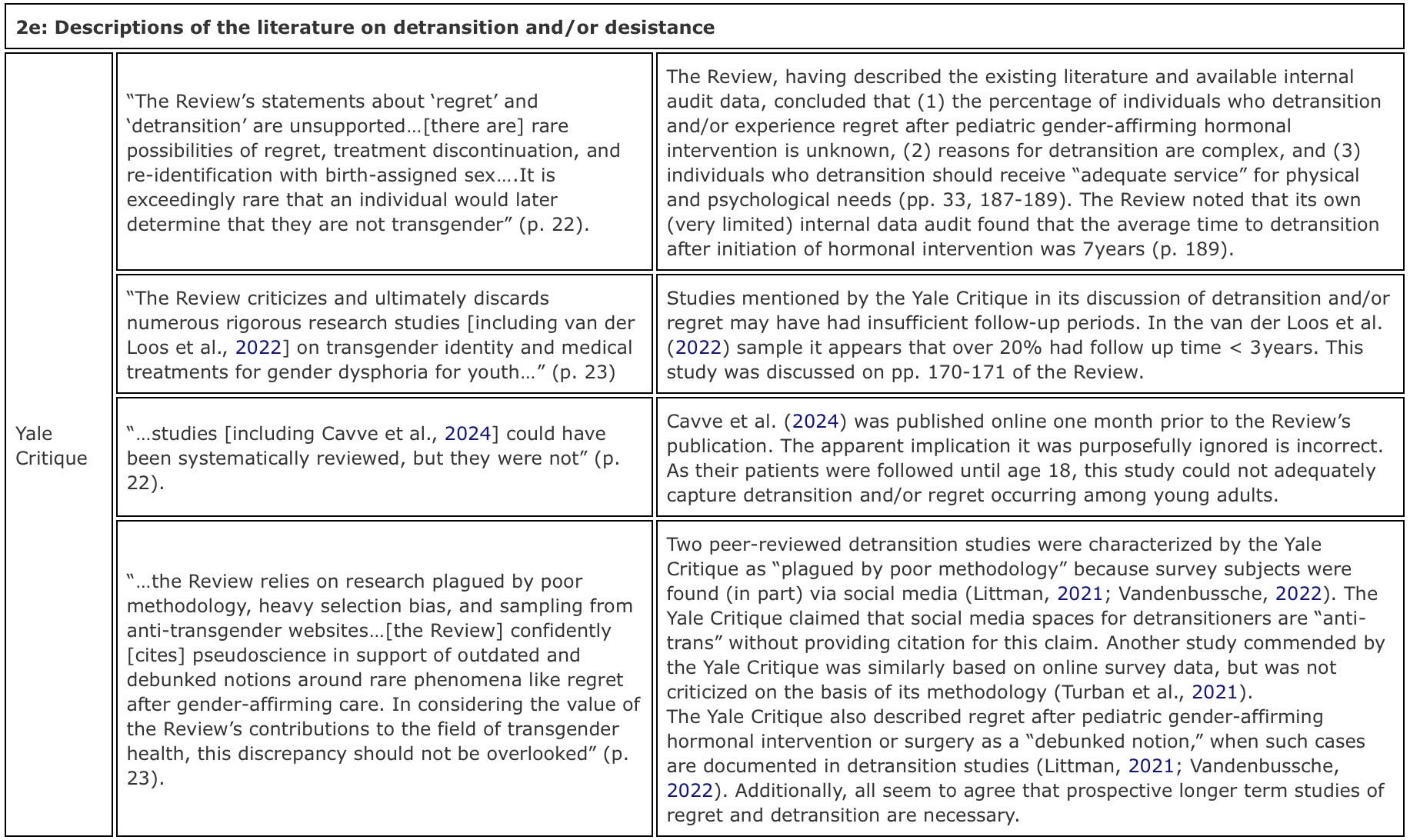
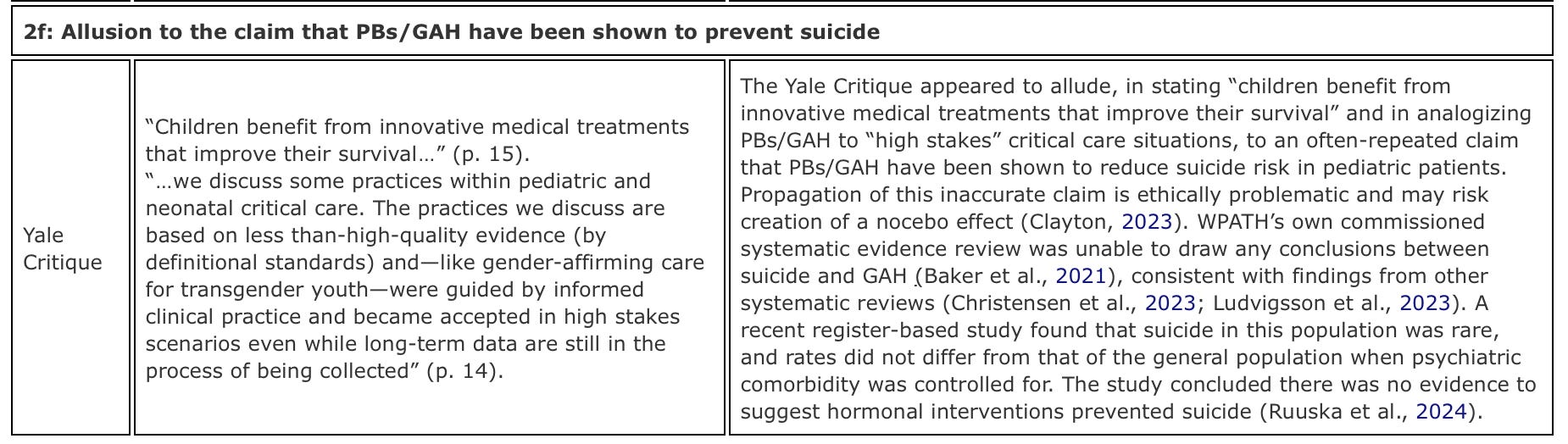
Metzger implied that valid and reliable arguments against the Cass Review exist. He’s wrong. Frequently gender affirmationists will trot out the online only not-peer-reviewed Yale critique, written by fanatical gender affirmationist activist researchers Meredithe McNamara, Joanna Olson-Kennedy, Jack Turban, and others. If you’ve been in this game long enough you recognise these names and you harbour heavy suspicion of them and legitimate skepticism about their work. You can read the analysis of the rebuttals here, by McDeavitt, Cohn, and Levine. I’ll share the tabular information which compares the misleading claims made in the Yale critique with an evidence and reality based response to the claims. Note, as SEGM noted, the Yale critique represents a veiled attempt to influence US litigation.

“There is no simple explanation for the increase in the numbers of predominantly young people and young adults who have a trans or gender-diverse identity, but there is broad agreement that it is a result of a complex interplay between biological, psychological and social factors. This balance of factors will be different in each individual.” — Cass Review, Final Report
I have a short clip specifically about Metzger explaining this and it will be the subject of a future article here.
Yes, let’s be honest and call things what they are, the paediatric GAC medical pathway is a a sex change for children. When we commit to dropping the euphemistic language used by the gender affirmation movement, we can begin to have honest conversations about what GAC really entails.
It’s medical experimentation, if we’re honest.