

“Puberty Blockers” Exacerbate Psychiatric Episodes :: Lupron Drug Monograph
so why are progressives insisting it’s a suicide prophylaxis for youth with G/D and a drug warranting Plan G coverage in BC

“Psychiatric events have been reported in patients taking GnRH agonists, including LUPRON DEPOT-PED. Postmarketing reports with this class of drugs include symptoms of emotional lability, such as crying, irritability, impatience, anger, and aggression. Monitor for development or worsening of psychiatric symptoms during treatment.” — Lupron Depot-Ped Clinical Studies, Lupron Depot Drug Monograph, Health Canada, Drug and Health Product Register, p. 16

As I’ve written previously, Lupron is a Plan G medication in BC. For readers who don’t know, Plan G is for provincial coverage of psychiatric medication.
According to the BC PharmaCare Policy Manual, “Plan G provides coverage of certain psychiatric medications to individuals for whom the cost of these medications is a serious barrier to treatment.” Also according to the PharmaCare Policy Manual, patients must meet the meet the following clinical eligibility for Plan G:
“without prescribed psychiatric medication, the patient is likely to be hospitalized for a psychiatric condition; OR
without prescribed psychiatric medication, the patient, or another person, is likely to suffer serious physical or psychological harm or economic loss”
There’s no clinical indication for treating gender dysphoria or gender discordance with Lupron. Repeat, it’s an off label use. There’s no valid and reliable evidence to support its use as a treatment for gender incongruence, Daniel Metzger and Jack Turban would have you believe otherwise, they will tell you that “puberty blockers” relieve suicidality and improve mood in young people experiencing psychological distress related to sexual development. They’ve medicalised normal adolescence, they’ve made puberty into some evil boogey monster that will kill young people.
I call horsesh1t. It’s simply untrue. Look at the long term historical picture of children and youth experiencing psychological distress and psychiatric events. There’s little evidence that adolescents needed any pubertal suppression to help them cope with the pressure of growing into a sexually mature body.
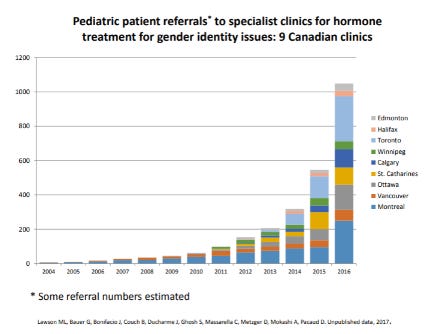
Ask yourself, when did this all started happening?
It began with the advent of SOGI. Numbers don’t lie, reader. Take a look. To understand this data it might help to know that Ontario introduced SOGI in 2015 and BC introduced it in 2016. We can easily surmise these numbers don’t tell the full story of demand for gender affirming care, because this data covers gender clinics and many young people don’t have access to gender clinics, they go to their paediatric or family doctor.
In his recent webinar presentation Metzger, admitted as much. It’s what Lisa Litmann’s research on ROGD revealed. Whilst Metzger denied the veracity of the ROGD research and dismisses it as a phenomenon, his “build it and they will come” argument to explain the precipitous rise in the demand for gender affirming care and gender clinics would seem to support the theory of ROGD.

Pedagogy training has become overly concerned with the pushing SOGI onto school aged kids, even as young as early elementary school.
Above you can see a YouTube video of a reading aloud of the children’s story Red: A Crayon’s Story. Written for children aged 4 to 8 years old and labeled preschool grade level by Amazon, the book, tells the story of a blue crayon with a red label. BCTF features Red: A Crayon’s Story in gender lesson plan resources. The lesson plan targets grades K-3 and 4-7.
“This is a lesson plan for teachers who may be new to teaching about gender identity and are looking for a safe way to explore the topic in class. This lesson uses the story “Red: A Crayon’s Story” to talk about feelings and attitudes that people could have in various situations. This activity is about showing diversity and showing that it is ok to be different.” — BCTF
What’s the message conveyed to children via this SOGI favourite?
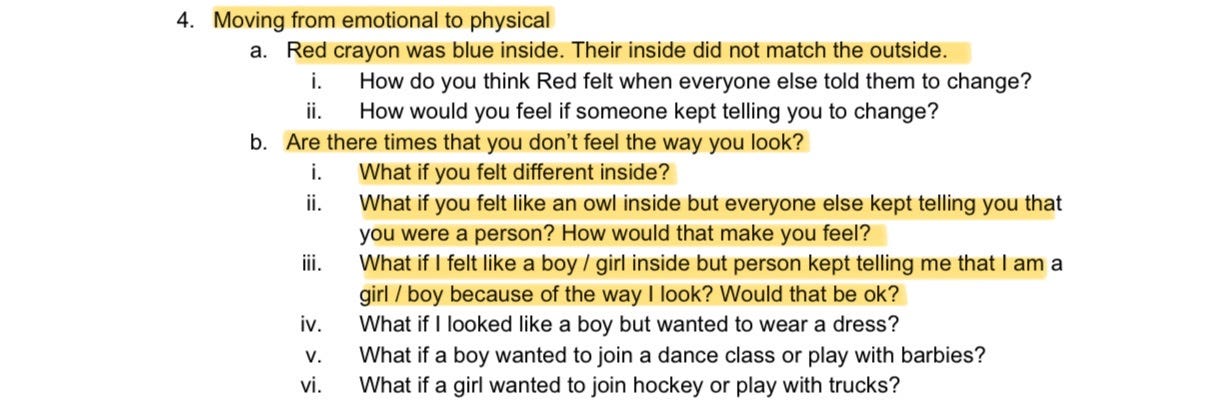
Well, that they could very well be in the wrong body. Maybe they’re a girl trapped in a boy body, maybe they’re a boy trapped in a boy body. This pedagogical philosophy reinforces gender stereotypes by implying that a boy who rejects boy activities and play might be a girl, and that a girl who rejects girl activities and play might be a boy. I cannot think of something more psychologically abusive than undermining a child’s sense of self at this level. Reader, take a look at the screenshot above from the lesson plan. What’s going on?
What does inside matching outside mean? What does not feeling the way you look mean? What does feeling like a boy/girl trapped inside a girl/boy body mean?
Their inside did not match the outside … Are there times that you don’t feel the way you look … What if you felt different inside … What if you felt like an owl inside but everyone else kept telling you that you were a person … What if I felt like a boy / girl inside but person kept telling me that I am a girl / boy because of the way I look?
Reader, this is NOT OKAY. It does not teach and promote personal self awareness. It does not teach social responsibility. In fact it reveals a high level of social irresponsibility and an egregious lack of self awareness on the part of educators who promote this as part of a healthy education.
When we have the BCTF promoting being a blue crayon with a red label to early elementary school kids as a safe and novel way to teach about “gender identity,” is it any wonder that the paediatric health care system has seen a precipitous rise in the demand for gender affirming care? Also reader, let’s be clear on the euphemistic language employed by the gender identity activism term for children sex change. “Gender affirming care” refers to paediatric sex change. “Puberty blocker” refers to chemical castration drugs.
The ACLU fights mandatory chemical castration for sex offenders as a human rights violation and also fights banning mandatory chemical castration for gender discordant kids. The reason you never noticed might have to do with the euphemism “puberty blockers” to describe admintering GnRHa to kids. It’s the same medication, reader.
The ACLU promoting experimental chemical castration treatment in vulnerable young people: “Having access to necessary care with trained professionals is lifesaving for young transgender people … For many young transgender people, gender-affirming care can typically include hormone treatment, puberty blockers, and counseling.”
The ACLU protecting the human rights of sex offenders to refuse chemical treatment: “While “chemical castration” may be a valuable tool in the fight to prevent sexual assault, the ACLU believes this legislation should be considered with extreme caution. The prospect of encouraging, perhaps even coercing, individuals to take drugs which alter their thoughts and behavior raises profound ethical and constitutional issues which cannot be ignored.”
Reader, in both cases the patient faces coercion to take GnRHa. The ACLU puts the individual freedoms of sex offenders ahead of public safety from sexual assault. They worry that it’s unethical to make a sex offender take a Gonadotropin hormone agonist, and they’re not worried about the ethics of making a vulnerable gender confused and emotionally distressed young person take a Gonadotropin-releasing hormone agonist. Do you see a problem here?
Yes, let’s sit here and pretend that it’s a TOTAL MYSTERY why the demand for services and paediatric gender clinics has sky rocketed throughout the 2010s. Yeah, I can’t figure it out, reader. (Sarcasm).
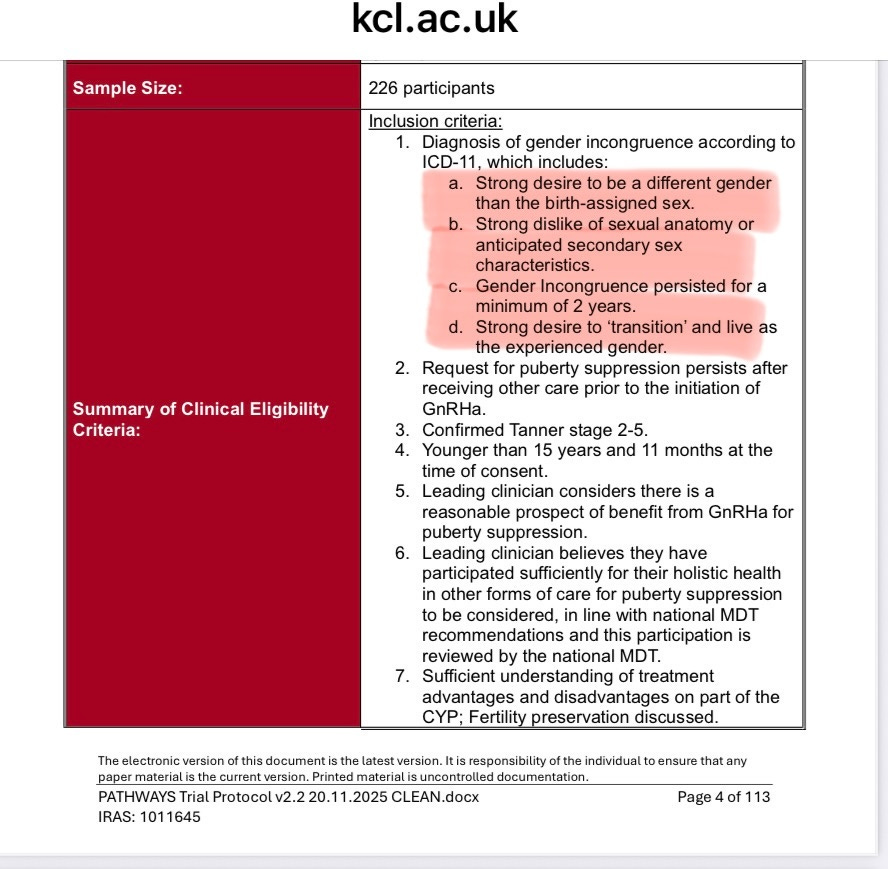
So, as the world wakes up to the dangers of paediatric gender affirming care, Canada continues to double down. And the UK decides to run a clinical trial for Lupron of n=226 kids with gender dysphoria. It baffles the reasonable mind.
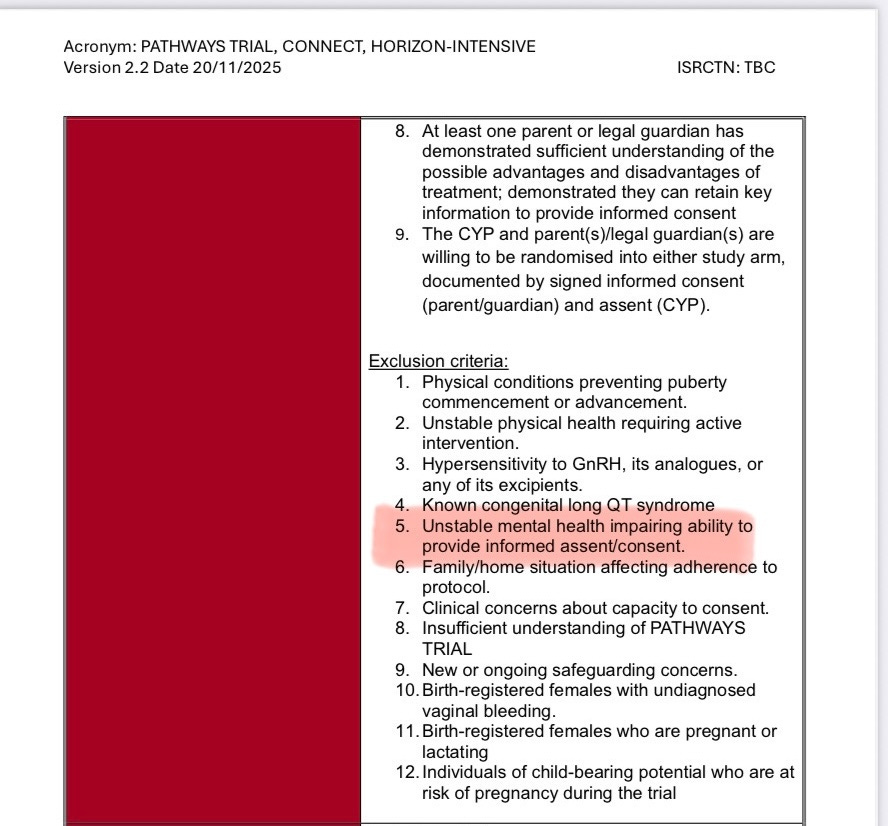
I’ll conclude with screenshots of the inclusion and exclusion criteria for the UK Lupron trial on gender dysphoric kids. It strikes me as having an unstable mental condition impairing consent when a child meets the diagnostic criteria for gender incongruence according to ICD-11. When a child expresses any of the following (below), they do indeed have an unstable mental health condition impairing their ability to provide informed assent/consent.
Strong desire to be a different gender than the birth-assigned sex.
Strong dislike of sexual anatomy or anticipated secondary sex characteristics.
Gender Incongruence persisted for a minimum of 2 years.
Strong desire to ‘transition’ and live as the experienced gender.
Remember, Lupron exacerbates and triggers psychiatric events, it doesn’t prevent or treat them.
“Psychiatric events have been reported in patients taking GnRH agonists, including LUPRON DEPOT-PED. Postmarketing reports with this class of drugs include symptoms of emotional lability, such as crying, irritability, impatience, anger, and aggression. Monitor for development or worsening of psychiatric symptoms during treatment.”